 |  |
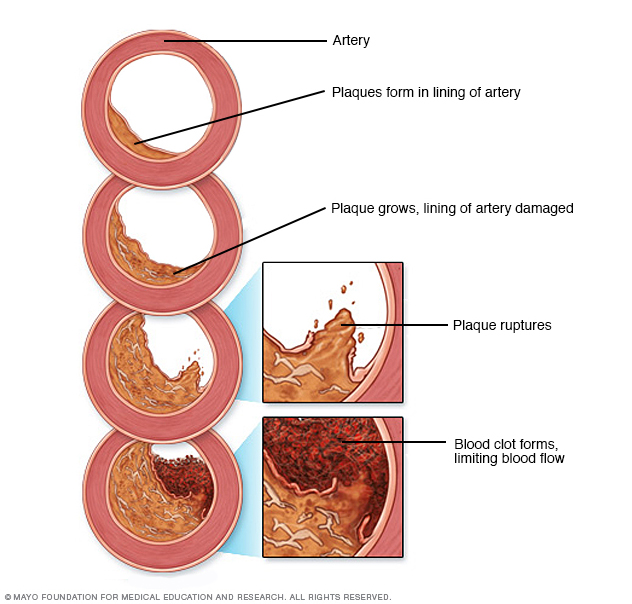
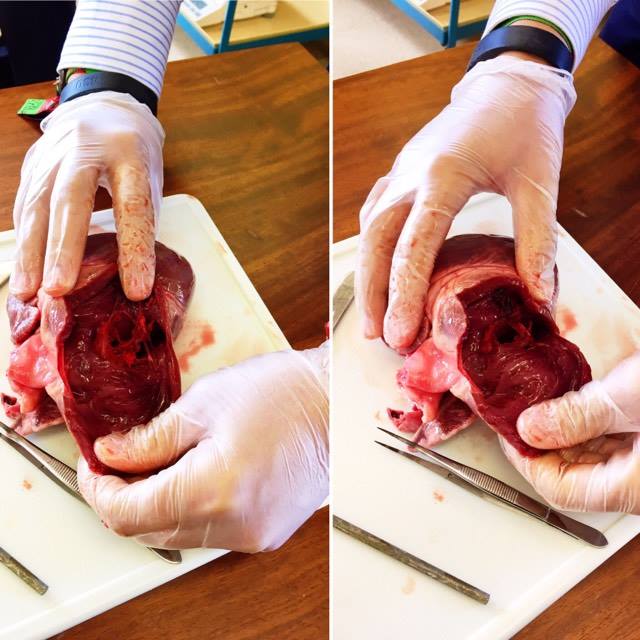
Coronary arteries are two large arteries that ascend from the aorta and supply the whole heart with blood. Occlusion means the obstruction, trapping of a liquid or gas. Thus, coronary occlusion is the blockage of a coronary vessel often by thrombosis or atheroma. This may cause myocardial infarction (heart attack). If the coronary arteries in your heart are narrow this consequently means that they cannot supply enough oxygenated blood to your heart. To begin with you may not experience any coronary artery disease symptoms however as the plaque increases the build up inside of the arteries you may develop the disease and symptom such as: Angina (chest pain) – This is a pressured tightness of the chest. Angina usually occurs in the middle left side of the chest and is normally triggered by emotional or physical stress. Shortness of breath – When your heart cannot pump enough blood to meet the requirement of the bodies needs then shortness of breath may develop as well as fatigue. Heart attack – If a coronary artery is completely and entirely blocked then it may cause a heart attack including pressure in the chest, pain in shoulder or arm, shortness of breath as well as sweating. However sometimes a heart attack can occur with no apparent signs or symptoms. Causes It is thought that damage to the inner layer of the coronary artery is what causes the disease however below are some other factors that may contribute:
Risk factors
Researches are finding that there may be other causes such as:
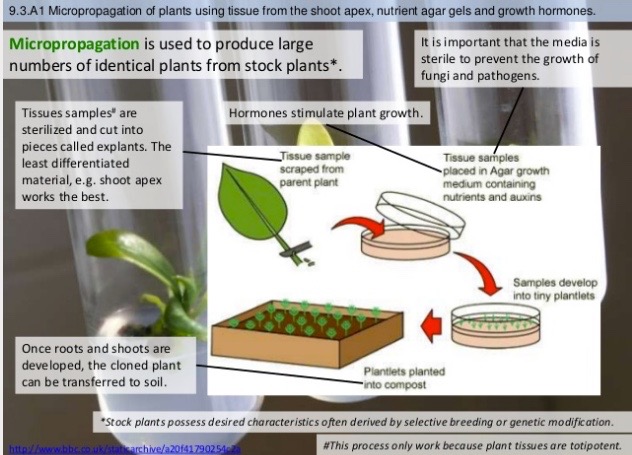
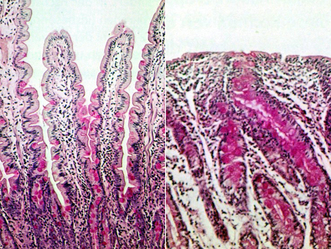
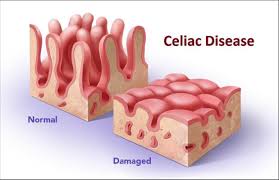
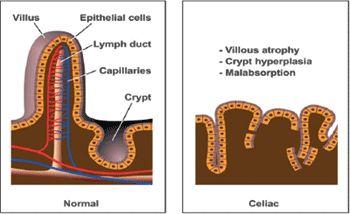
Points to be addressed: What is coeliac disease? Describe the basic causes and symptoms of coeliac disease Explain the effect of coeliac disease on intestinal villus and how this leads to its symptoms Describe the effect of genetics on a persons predisposition to coeliac disease Coeliac disease is a chronic autoimmune condition where a person has an adverse reaction to gluten. Symptoms can be: diarrhoea, bloating, flatulence, feeling fatigue all the time (this is as a consequence of malnutrition, not receiving enough nutrients from food), and if a child, not growing at the expected rate. Coeliac disease is not an allergy not intolerance to gluten. It is an autoimmune condition meaning the immune system mistakenly attacks healthy tissue. The immune system of someone who has coeliac disease accidentally mistakes the substances within gluten dangerous to the body and attacks. This reaction causes damage to the surface of the small intestine, disrupting absorbance of nutrients from foods (which is why malnutrition may be a symptom). The reason behind the immune system's reaction to gluten is still not entirely clear however it is known that a person genetic makeup as well as the environment have an effect. The immune system produces antibodies in order to "fight off" a substance called gliodin, which is found within gluten. These antibodies which are produced irritate the surface of the intestine causing it to become red and inflamed (red and swollen). Villi covers the surface of the small intestine in order to increase the surface area for absorption of nutrients. However as a consequence of coeliac disease the inflammation and swelling flattens the villi limiting their him in absorption. Consequently this means digestion is affected leading to as I said before inefficiency of absorbance of nutrients leading to the symptoms listed above. It has not been discovered fully why some people have coeliac disease or the reasons behind why some people have mild symptoms and others severe. Although there are some factors which can increase the chances of coeliac disease. Family history increases the chance of coeliac disease. Family history increases the chance of having coeliac disease by 10%, more so if you have an identical twin 75%, that you will also develop the condition. Research has provided evidence that the disease is associated with a number of genetic mutations affecting a group of genes called the HLA-DQ genes. These genes are responsible for the development of the immune system. The fact that these mutations occur in about 1/3 of the population suggests that perhaps there is something else, such as environmental factors also playing a part. Environmental factors are thought to play a role in coeliac disease. Through introducing gluten to a baby's diet before they are three months old may increase the risk of developing coeliac disease. Doctors and experts say not giving your baby/child gluten until at least six months old. If the baby is not breastfed whilst gluten has been introduced this is also thought to increase chances. Although there is not direct cure for coeliac disease there is treatment. For example switching to a gluten free diet. This is recommended to remove gluten from your diet no matter the severity of the condition. Testing for coeliac disease is done through 'screening' this is usually only recommended for those who have a history of coeliac disease within their family. Blood tests can also be done to determine if a person may have coeliac disease. A biopsy is then completed in order to confirm the diagnosis of the blood test.
 Olaf loved adventures. By the age of six Olaf discovered what he truly wanted to do... He knew what the ultimate adventure would compromise of. But who would he go with? He pondered. Not Nicky nitrogen, nor Aaron argon, definitely not Chuck carbon dioxide. "I must go alone" he reluctantly told himself. Olaf closed his eyes hoping for the best. A deep slumber took over. Olaf was asleep.
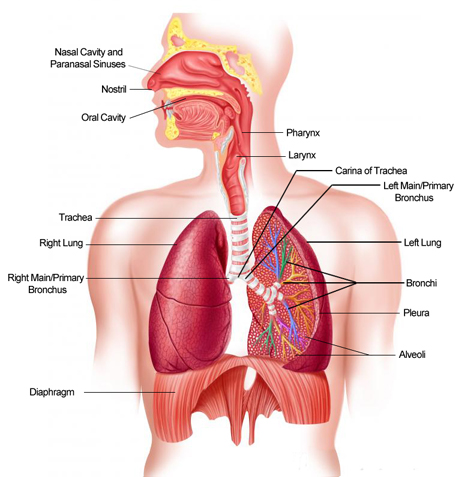
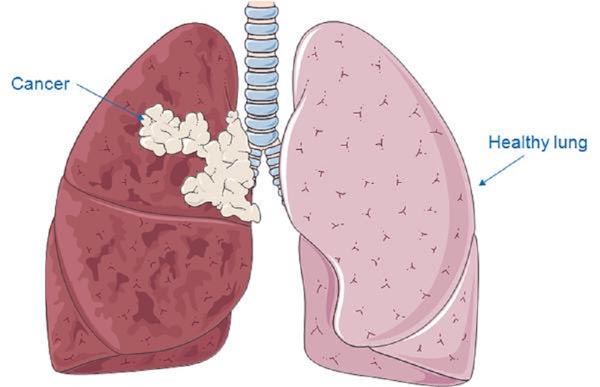
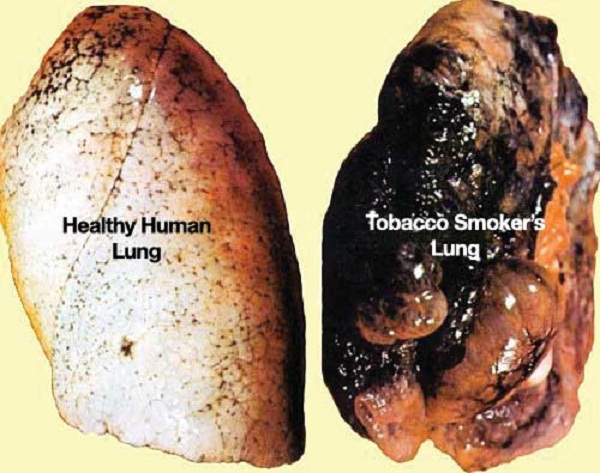
Suddenly, Olaf was being sucked into a tubular like construction he had never seen before. Warmth and a certain dampness surrounded him. He was pulled down the continuous tube. Olaf tried to resist, but his attempt failed; he was too weak. Succumbing to the powerful force he found himself travelling into a larger tube. This time he was not alone... Dark shadows came from above. A huge bolus of food hit Olaf. Gulping filled his ears. Bolus after bolus Olaf was beaten again and again. Flinching away he found himself in a new, tighter tube. Olaf felt alone. For the first time in his life he dreamed of being somewhere familiar. Would he ever see his family again? His wife? His children? His bakery... A tear streamed down Olaf's cheek that was damp from perspiration. "Hi!" an unfamiliar voice nearing him exclaimed. "Look, it's okay, don't cry, you aren't-" Olaf wiped away his tears and opened his eyes. Before him stood a young lady by the name of Olafa. "Please don't cry." Empathy filled her voice. "I'm just so scared - sorry, what's your name? I should introduce myself." Olaf's cheeks turned pink with embarrassment. "I'm Olafa, I've been through this before" "Been through what before?" Olaf questioned. "The respiratory system silly" The respiratory system. Olaf's eyebrows knotted together in confusion. Olafa knew from the puzzled expression on his face that Olaf had no recollection of what she was on about. "Well listen up Olaf, you're about to learn. First you were sucked into what is called a nose, you then travelled into the pharynx where i saw you beaten by food, luckily the pharynx separates into two tubes, one to the stomach and the other to the lungs which is where we are headed now." She signed. Olaf nodded his head he had not heard one word of what she had said for he found himself in a trance, mesmerised and lost in her deep blue eyes. Olaf and Olafa found themselves deep in conversation as they travelled through the trachea, a passageway connecting the larynx to the lungs. He was a baker and she was a biologist. Worlds apart fate had brought them together in this mystical terrain he had never experienced before known as 'The Respiratory System'. Olaf no longer felt alone, Olafa reassured him and led him to the bronchi. Two tubes appeared before the two who were completely and utterly engrossed in one another. He grabbed her hand and intertwined his fingers with hers. Olaf's wife no longer had any significance. They travelled down the right bronchiole, hands clasped. He glanced up and their eyes met. He felt butterflies from within. How could something so wrong feel so right? Tiny sacs surrounded them. Through the bronchiole and into the lungs they went. A large structure beneath was contracting and expanding. Olaf's heart began to beat faster each moment. "That's called the diaphragm, it's the only muscle in the respiratory system" Olafa informed him. She was both beauty and brains. Their fingers parted and before he knew it she was gone. Squeezing through the alveoli Olaf began to feel panicked. Capillaries were everywhere. Lost in a bed of capillaries Olaf tried to calm himself. The surface area was so huge, there was no way he would ever find her again. Reminiscing over the past moments of his life, Olaf realised he had never felt like this before. He could not let her go. Olaf frantically pushed through the capillaries in hope of finding Olafa. The red blood cell came to a sudden halt. What he saw before his eyes was terrifying. He pinched himself to try and rid himself of this horrific nightmare. Olaf could no longer breathe, a pressure was against his chest compressing his entire body. His body was being squeezed into a single pulp. His electrons being pulled away from him reducing him to nothing more than a meaningless nucleus. The physical strain on his inevitably disintegrating drained body was no match for the psychological pain embedded within his baker brain. If Olaf died now he had experienced the ultimate adventure at last. The respiratory system had breathed life into him like never before, showing him things he had never witnessed. Introducing him to Olafa; simply the greatest moment of his life. He would never forget. His life was slowly slipping away, thus he could not grasp it. S U D D E N L Y , Olaf's eyes flashed open! Light flowing in causing him to flinch after the sudden intake of photons. Pressed against a gel like membrane Olaf was trapped. Squinting his eyes Olaf made sense of a faint figure in the distance. Peering through the phospholipid bilayer it became apparent that Olafa, too, was trapped within the membrane of a neighbouring cell. He wanted to cross. He wanted to see her. The very thing that had brought them together was now separating them, the respiratory system. And so, a mitochondria came along, sweeping Olaf away to break glucose up. Olaf of house montague and Olafa of house capulet were never to see eachother again. LUNG CANCERSYMPTOMS Although there are no clear signs in the early stages of lung cancer the following are often developed throughout the condition: - a persistent cough - coughing up blood - constant breathlessness - fatigue - weight loss - ache/pain when breathing/coughing CAUSES The biggest cause of lung cancer is smoking. It is known to cause 86% of lung cancer cases, including second hand smoke, passive smoking. Both the length of time you have been smoking and the number of cigarettes smoked per day have a negative effect on your health. The younger you start smoking, the more threatening it can be, (if you start smoking as a child it is more dangerous than starting as an adult). Quitting smoking will decrease the chance of getting lung cancer. Passive smoking can have an effect on the lungs causing damage. Smoking is not the only cause of lung cancer however it is the predominant one. There are other factors which affect the chances of lung cancer such as exposure to radon gas and certain chemicals, being immersed in an environment with high air pollution, previously having a lung disease, past cancer treatment, previous cancers that have been smoking related as well as lowered immunity. These other factors do not play such an important role in causing lung cancer as smoking does. Radon Gas - naturally occurring gas present in uranium found in rocks. The gas can build up inside buildings and homes consequently damaging peoples lungs in small amounts. After smoking radon is one of the greatest causes of lung cancer. Biological consequences of lung cancer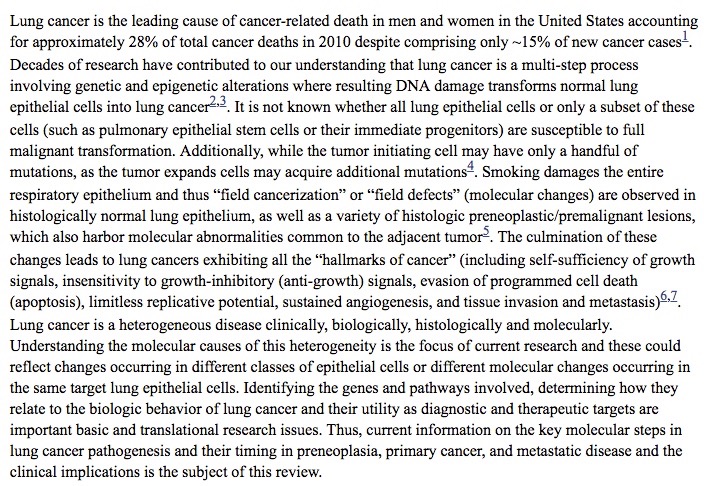 Approximately 85% of lung cancers are caused by carcinogens present in tobacco smoke, while worldwide, 15–25% of lung cancer cases occur in life time “never smokers” (less than 100 cigarettes in a lifetime). These etiologic differences are associated with distinct differences in tumor acquired molecular changes and are discussed later in this review9,10. While the general public associates lung cancer with smoking, due to the number of lung cancer cases overall, lung cancer occurring in life time never smokers is also a huge public health problem. Likewise, over 50% of newly diagnosed lung cancers in the USA occur in “former smokers” who changed their lifestyle – but the damage caused by past smoking still led to the development of lung cancer. Thus, it will be important to identify the non-smoking related etiologies of lung cancer arising in “never smokers” as well as methods to identify which former smokers are most likely to develop clinically evident lung cancer. Scagliotti GV, Longo M, Novello S Curr Opin Oncol. 2009 Mar; 21(2):99-104.
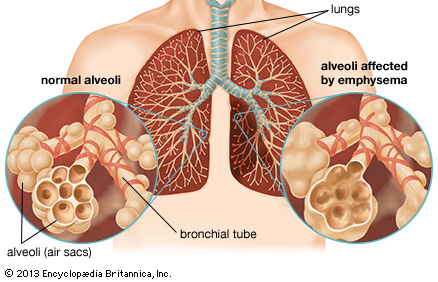
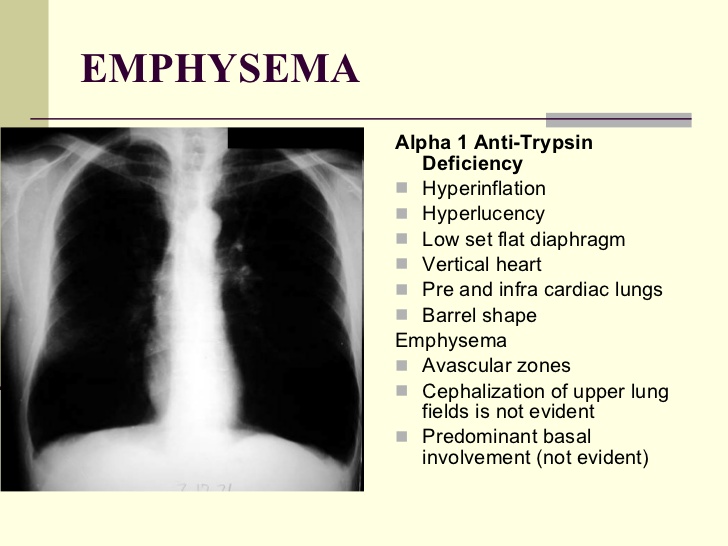
EMPHYSEMASYMPTOMS The most common symptom of emphysema is shortness of breath. This is due to the structural changes of the lungs most commonly as a consequence of smoking. - wheezing - coughing - chest tightness or pain - loss of appetite as well as weight loss - depression - poor sleeping quality - decreased sexual function Similarly to lung cancer, the symptoms are more common and recognisable when in the advanced stages in comparison to the early stages. The symptoms of emphysema are progressive thus meaning they get worse as time increases. Like lung cancer, emphysema is mainly caused by smoking. In addition to smoking some other causes are smoking marijuana, air pollution and manufacturing fumes. Finally emphysema can be passed on by a deficiency of a protein that protects the elasticity of structures within the lungs, alpha 1 anti-trypsin deficiency emphysema.
As we grow older our lungs slowly lose their function. In emphysema the persons lungs function is lost at an accelerated rate.
In smokers who develop emphysema the symptoms are often present from ages 45-60. Scientists and doctors still have a lot to learn about why emphysema appears and within who. It is believed however that genetic factors can play a role, for example genetic factors may cause the symptoms of emphysema to develop faster in some than in others. Emphysema gradually damages the alveoli in your lungs. Alveoli are air sacs. Emphysema is classed as a COPD, chronic obstructive pulmonary disease. The alveoli are grouped together in the lungs like a bunch of grapes. When someone has emphysema the inner walls of the alveoli begin to break down and rupture which consequently creates one large air space defeating the purpose of the structure of the alveoli. Protease is released by leukocytes in the lungs which breaks down the tissue. The rupturing of the alveoli walls causes a decrease in the surface area consequently limiting the rate of gas exchange and oxygen passing into the bloodstream, this explains the symptoms such as shortness of breath. Each breath out leaves the air trapped inside of the damaged alveoli meaning there is no fresh oxygen to be breathed in. The breakdown of the alveoli walls affects the surface area limiting the amount of oxygen into the bloodstream causing the shortness of breath and other symptoms. BIBLIOGRAPHY: www.mayoclinic.org/diseases-conditions/emphysema/basics/definition/con-20014218 www.cancerresearchuk.org/about-cancer/type/lung-cancer/about/lung-cancer-risks-and-causes www.nhs.uk/conditions/Cancer-of-the-lung/Pages/Introduction.aspx www.ncbi.nlm.nih.gov/pmc/articles/PMC3367865/ www.mayoclinic.org/diseases-conditions/emphysema/basics/risk-factors/con-20014218  Kristin Winchell from the University of Massachusetts and her team investigated male anole lizards (Anolis cristatellus) in Puerto Rican cities of Mayaguez, Ponce and San Juan in comparison to those of nearby forests. Her team were inspired to begin research after she "chased a lizard that ran straight up window 30 feet and was out of reach in 15 seconds". The results of the findings were that city lizards were found to be able to cling to flat objects, such as walls and windows. This evolved ability means they can use the full urban environment instead of restricting themselves to forest like environments. Another finding was that city lizards had longer limbs with scale like structures referred to as lamellae (which help their toes stick to surfaces). These traits have enabled the lizards to attach themselves to the many slippery surfaces found in an urban scene. “Urban areas are just another environment,” Winchell says. “The animals that live there aren’t somehow immune to natural selection.” The team also raised urban and forest lizards from the Mayagüez region in the lab and found that differences in limb length and scale number remained, suggesting a genetic basis to the urban lizards’ abilities. Winchell says understanding urban adaption could help conservation. “Having a grasp on which animals tolerate urbanisation gives us a better idea of which ones we need to focus on when preserving natural habitats,” she says. - New Scientist This article appeared in print under the headline “Lizard’s feet have evolved to let it race up windowpanes” 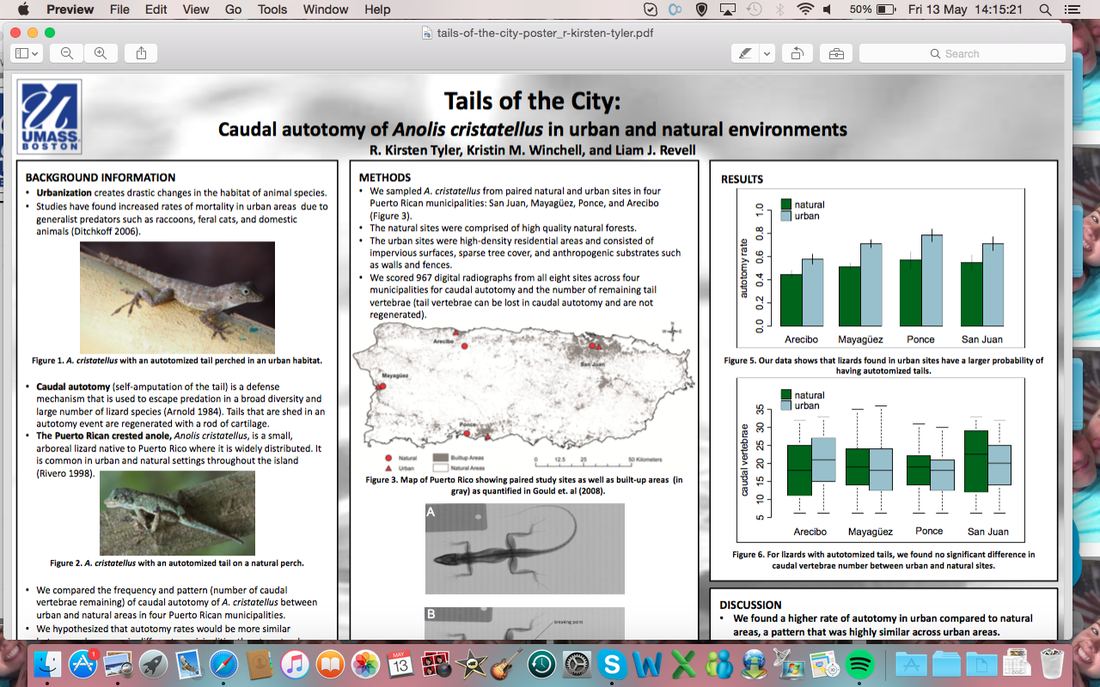 |

Professor Laura M TotterdellPhD in physiology and cake making as well as quantum physics. Archives
April 2016
Categories |





 RSS Feed
RSS Feed
